Headaches are one of the most common complaints in outpatient and emergency settings. Almost everyone experiences them at some point. Yet when it comes to documentation and coding, a simple “headache” ians never just simple. Coding it incorrectly can lead to denials, downcoding, or even audit risk. That is why understanding how to use ICD-10 code R51 correctly matters more than most providers realize.
In the United States, diagnostic coding follows the official structures of the Centers for Disease Control and Prevention and the Centers for Medicare & Medicaid Services. Headache coding sits under the broader ICD-10-CM classification system, which impacts medical necessity, reimbursement, and claim approval. Let’s break it down in practical terms.
Understanding ICD-10 Code R51
ICD-10-CM code R51 historically represented “Headache.” However, coding updates refined this category. Today, the classification includes:
- R51.0-Headache with orthostatic component
- R51.9-Headache, unspecified
That shift was not cosmetic. It changed documentation expectations and claim accuracy. When providers continue using unspecified diagnosis codes without specificity, payers often flag the claim for medical necessity review.
Headaches are classified under Chapter 18 of ICD-10-CM: Symptoms, Signs, and Abnormal Clinical and Psychological Findings. That means R51 codes describe symptoms, not definitive neurological diagnoses. And that distinction is critical.
When To Use R51?
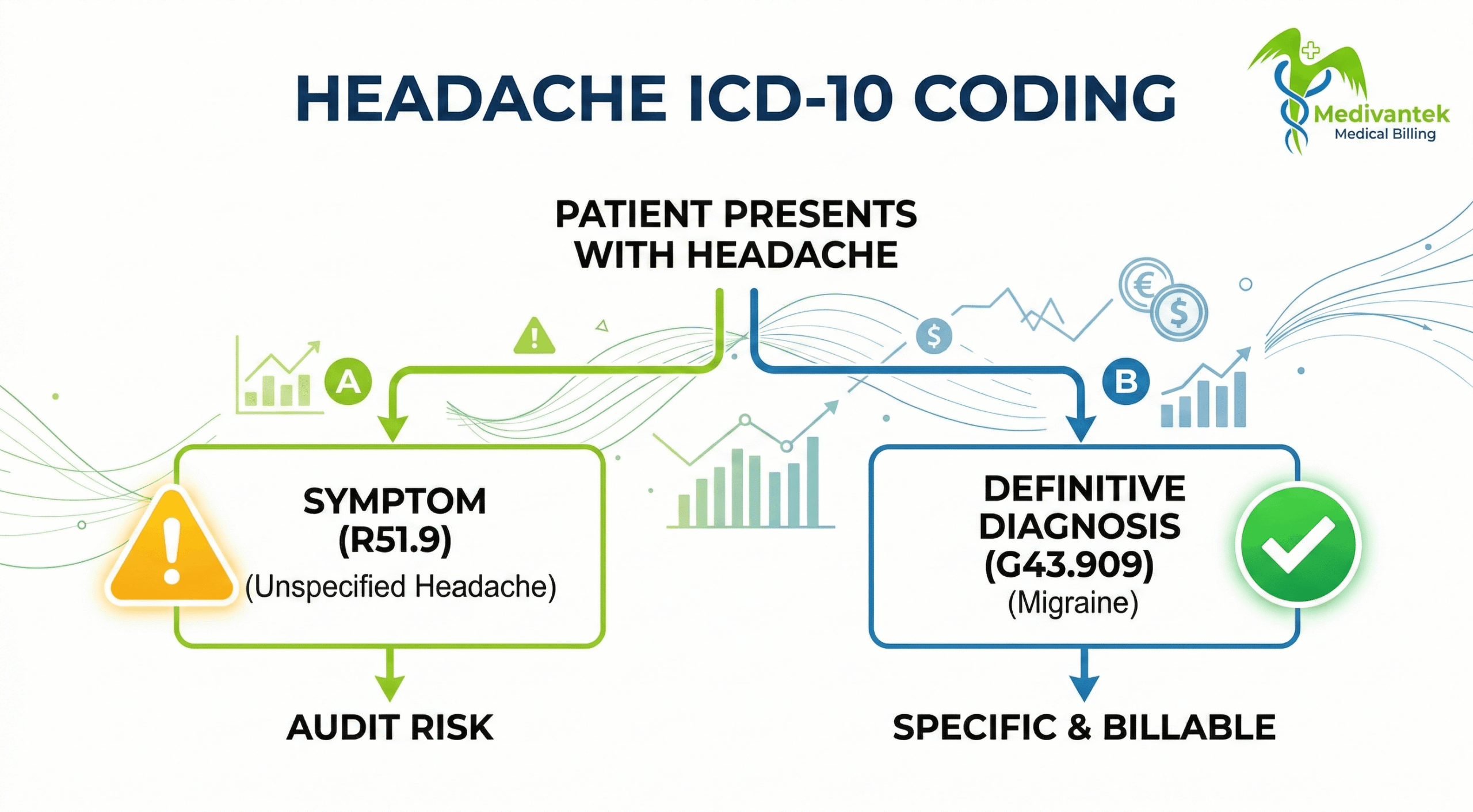
R51 should be used only when the provider has not determined a specific headache type. For example, if a patient presents with “diffuse head pain” and no diagnostic conclusion is reached, R51.9 may be appropriate.
However, if the provider documents:
- Migraine
- Cluster headache
- Tension-type headache
- Post-traumatic headache
Then, the symptom coding is no longer correct. Instead, you must code the definitive diagnosis from Chapter 6 (Diseases of the Nervous System).
This is where many practices slip. They default to R51 even when documentation supports a more specific code.
Migraine vs. Unspecified Headache
For example, migraines are coded under G43 categories. If a provider diagnoses migraine without aura, unspecified, the correct code is G43.909. Using R51 instead would be inaccurate and may affect reimbursement.
Insurance carriers review medical necessity based on the specificity of the diagnosis. For imaging studies such as CT scans or MRIs, an unspecified headache typically does not warrant advanced imaging unless red flag symptoms are documented.
Commercial payers, Medicare, and Medicaid all scrutinize unspecified symptom codes more closely today.
Clinical Documentation Requirements
Accurate coding always begins with documentation. Providers must clearly record:
- Onset (sudden vs gradual)
- Duration
- Location (frontal, occipital, unilateral)
- Severity
- Associated symptoms (nausea, visual changes, photophobia)
- Aggravating or relieving factors
If orthostatic features are present, documentation must support positional worsening to justify R51.0. Incomplete notes lead to incorrect coding. Incorrect coding leads to denials. It’s a domino effect.
Medicare and Payer Considerations
Under the Medicare Physician Fee Schedule (MPFS), reimbursement depends on both CPT and ICD-10 pairing. Medicare expects diagnostic specificity.
If a patient presents with chronic daily headaches, coding only R51.9 repeatedly without further evaluation may trigger audits. Medicare often expects workup progression.
Commercial carriers sometimes deny imaging when only R51.9 is listed without neurological deficits. State Medicaid programs also monitor frequent symptom coding. Repeated unspecified symptom claims can signal quality concerns.
Fee Schedule and Revenue Impact
Headache visits are often billed using E/M codes (99202-99215, depending on setting). The relative value units (RVUs) assigned under MPFS determine reimbursement.
For example:
- Low complexity headache visit = lower RVUs
- Headache with neurological evaluation and imaging decision = higher RVUs
But diagnostic specificity supports higher levels of medical decision-making. If documentation shows complex migraine management but coding uses R51.9, reimbursement may not reflect the true complexity.
Headache visits may look routine. A patient walks in with pain. The provider evaluates. Medication is prescribed. The claim goes out.
Headache ICD-10 Code Billing Process
But when you dig deeper, headache encounters often involve imaging, neurological evaluation, medication management, or specialist referrals. That means higher scrutiny from payers. If your workflow is sloppy, denials follow quickly.
Below is the entire billing cycle from front desk to final payment.
Step 1: Eligibility Verification and Benefit Confirmation
Everything starts before the patient even sees the provider.
Eligibility verification is not just confirming that the policy is active. It means confirming:
- Plan type (HMO, PPO, Medicare Advantage, Medicaid)
- Copay, deductible, and coinsurance
- Imaging coverage
- Specialist referral requirements
- Prior authorization rules
Headache complaints often lead to CT or MRI scans. Commercial carriers frequently require prior authorization for advanced imaging. Medicare typically does not require traditional prior authorization for imaging, but medical necessity must be clearly documented under policies influenced by the Centers for Medicare & Medicaid Services.
If imaging is performed without authorization when required, the denial is almost guaranteed. Appeals rarely succeed. Front-desk accuracy protects backend revenue.
Step 2: Documentation and Diagnosis Coding
Once the visit is complete, documentation becomes the foundation of billing.
The provider should clearly document:
- Onset and duration
- Location and severity
- Associated symptoms (nausea, photophobia, aura, neurological deficits)
- Past headache history
- Clinical decision-making
The coder’s job is to accurately translate documentation into ICD-10 codes. If the provider diagnoses migraine, tension-type headache, cluster headache, or post-traumatic headache, those specific neurological codes must be used. If no definitive diagnosis is reached, R51.9 (Headache, unspecified) should be assigned only then.
Here’s where many practices make mistakes. They default to R51 even when documentation supports a more specific diagnosis. That weakens medical necessity for imaging and may reduce reimbursement support for higher-level E/M coding. Specificity matters.
Step 3: CPT Coding and E/M Level Selection
Now we move into procedural coding. Most headache visits involve evaluation and management (E/M) services.
Under current E/M guidelines, the visit level depends on medical decision-making or total time spent. Ordering imaging increases complexity. Reviewing prior scans increases complexity. Managing chronic migraines with medication adjustments increases the risk level.
If the documentation supports moderate medical decision-making, the CPT code should reflect that. Underbilling leaves revenue on the table. Overbilling invites audits.
The key is alignment. The diagnosis, documentation, and E/M level must all tell the same clinical story.
Step 4: Claim Submission
Clean claims move faster. Before submission, verify:
- Correct ICD-10 to CPT linkage
- Accurate provider NPI and taxonomy
- Proper place-of-service code
- Modifiers if applicable (e.g., 25 modifier if a procedure is performed on the same day as an E/M visit)
If imaging is performed in-office, global billing rules must be followed. If interpretation is separate, professional and technical components must be coded correctly. Small data entry errors delay payment. A structured pre-submission review process dramatically reduces rejection rates.
Step 5: Payer Adjudication
Once submitted, the payer reviews the claim.
If the diagnosis is unspecified and a high-cost service, such as an MRI, is billed, the claim may be flagged. Payers often request medical records to confirm medical necessity.
Medicare Administrative Contractors evaluate claims based on local coverage determinations. Commercial carriers use internal clinical guidelines.
If documentation lacks red flag symptoms such as neurological deficits, sudden onset (“thunderclap” headache), trauma, or systemic symptoms-imaging may be denied as not medically necessary. This is where documentation strength determines revenue success.
Step 6: Payment Posting and Reconciliation
Once payment arrives, post it accurately. Compare allowed amounts to contracted rates. Identify underpayments. Review adjustments carefully.
Headache visits may involve multiple line items: E/M, imaging, and injections. Each must reconcile properly. Ignoring small discrepancies adds up over time.
Step 7: Denial Management and Appeals
If the claim is denied for lack of medical necessity, do not panic. Start with root-cause analysis.
Ask these questions:
- Was a more specific diagnosis documented but not coded?
- Were red flag symptoms documented clearly?
- Was prior authorization required and missed?
- Was the E/M level justified?
If documentation supports medical necessity, submit a corrected claim or formal appeal with clinical notes attached. Strong appeals cite documentation clearly and reference payer policy language when possible. Vague appeals rarely succeed.
Headache Billing Errors and How to Fix Them
Headache encounters are common. In primary care alone, millions of visits every year involve some form of head pain. Because volume is high, even small billing mistakes multiply quickly. One was denied an MRI here. One downcoded E/M there. Before you know it, revenue starts leaking.
Most problems do not come from complicated regulations. They stem from minor oversights in documentation, coding, or the front-end workflow. The fix is rarely dramatic. It is usually about tightening processes and educating teams.
Below are the most frequent errors in headache-related billing and, more importantly, how to fix them properly.
Overuse of R51.9 (Headache, Unspecified)
This is the classic mistake. The provider documents “headache.” The coder assigns R51.9 without digging deeper. The claim goes out. It gets paid sometimes.
But when imaging is ordered, or when the visit level is higher, payers start questioning medical necessity. Repeated use of unspecified codes is a red flag for insurers. Contractors working under policies influenced by the Centers for Medicare & Medicaid Services often analyze patterns. If 70-80% of your headache claims use R51.9, your documentation quality may be reviewed.
How to Fix It Train providers to document headache type clearly. Migraine. Tension-type. Cluster. Post-traumatic. Medication-overuse headache. Even one additional sentence in the assessment section can shift coding from unspecified to a more accurate neurological diagnosis. Coders should also review the medication list. If triptans are prescribed, migraine is likely documented somewhere. Match coding to documentation, not assumptions.
Imaging Ordered Without Strong Medical Necessity
CT scans and MRIs drive revenue. They also drive denials. Payers expect documentation of red flags before approving advanced imaging for headache. Examples include:
- Sudden onset of severe headache
- Neurological deficits
- Head trauma
- Cancer history
- Signs of infection
If imaging is ordered for routine chronic headaches without documented change in pattern or severity, denials are common.
How to Fix It Ensure documentation clearly supports why imaging is necessary. The note should explain clinical reasoning, not just “rule out pathology.”
Incorrect E/M Level Selection
Headache visits range from simple medication refills to complex neurological evaluations. Under current E/M guidelines, level selection depends on medical decision-making or time. Yet many providers under-document complexity. Others overcode without adequate support.
For example: If the provider reviews prior imaging, adjusts medication, discusses risks, and evaluates new symptoms, that likely supports moderate complexity. If documentation only states “continue medication,” it supports a lower level. A mismatch between documentation and CPT level invites audits.
How to Fix It Educate providers on documenting medical decision-making elements clearly:
- Number and complexity of problems
- Data reviewed
- Risk of management decisions
Coders should validate every higher-level E/M code before claim submission. Internal audits help identify patterns early.
Missing Modifier 25 When Appropriate
If a procedure is performed on the same day as an evaluation visit, modifier 25 may be required. For example, if a patient presents with a headache and receives a trigger-point injection during the same visit, the E/M service must be separately identifiable, and modifier 25 must be appended.
Failure to append modifier 25 results in bundling denial. Overuse of modifier 25 without documentation support, however, raises compliance risk.
How to Fix It Document the separately identifiable evaluation clearly. The note should show a distinct assessment beyond the procedure itself. Review National Correct Coding Initiative (NCCI) edits before submission.
Failure to Code Associated Conditions
Headaches often coexist with other conditions, such as:
- Hypertension
- Sinusitis
- Depression
- Cervical spine disorders
If these conditions are evaluated and managed during the encounter but not coded, the claim may underrepresent complexity. That affects reimbursement and can weaken medical necessity arguments.
How to Fix It Code all documented and clinically addressed conditions that impact care during the visit. Avoid coding irrelevant history-only conditions. Stick to what is evaluated, assessed, or treated.
Authorization Errors for Referrals and Imaging
Many headache visits result in referrals to neurology or imaging studies. If the patient’s plan requires a referral from a primary care provider and it is missing, claims may be denied outright. Front-desk verification errors create backend chaos.
How to Fix It Implement a checklist during eligibility verification:
- Confirm referral requirement
- Confirm prior authorization requirement
- Confirm network status
Do not assume. Always verify.
Weak Denial Follow-Up
Denials happen. The bigger issue is failing to respond properly. Many practices write off headache imaging denials without reviewing documentation. That is lost revenue. Often, documentation supports medical necessity but was not submitted initially.
How to Fix It Create a structured denial management workflow:
- Identify the denial reason code
- Review documentation
- Correct coding if needed
- Submit an appeal with supporting notes
Track denial trends monthly. If imaging denials increase, it signals gaps in documentation or authorization.
Poor Documentation of Chronicity
Chronic migraines require ongoing management. If documentation does not show progression, medication changes, or reassessment, repeated visits may appear unnecessary to payers. Patterns matter.
How to Fix It Encourage providers to document:
- Frequency of episodes
- Response to treatment
- Changes in pattern
- Functional impact
Clear follow-up documentation supports continued medical necessity.
Final Thoughts
Headache coding may look straightforward. In reality, it requires attention to detail, updated knowledge, and strong documentation practices. Using R51 correctly ensures accurate reimbursement, supports medical necessity, and protects compliance. Precision always pays off in medical billing.
Stop Headache Billing Errors Before They Impact Revenue
Accurate headache coding goes far beyond assigning ICD-10 code R51. Documentation gaps, incorrect diagnosis selection, imaging denials, and E/M mismatches can silently reduce reimbursements and increase audit exposure.
Medivantek Medical Billing Services helps healthcare providers strengthen revenue performance through:
- Accurate ICD-10 & CPT coding alignment
- Medical necessity validation for imaging claims
- E/M level optimization
- Denial management and appeals support
- End-to-end Revenue Cycle Management (RCM)
Schedule a Free Billing Assessment with Medivantek Medical Billing Services and discover opportunities to improve reimbursement accuracy and reduce claim denials.