Headaches are one of the most common complaints in outpatient and emergency settings. Yet when it comes to documentation and coding, a simple “headache” is never just simple. Coding it incorrectly can lead to claim denials, downcoding, and increased audit risk.
Because headache coding falls under the broader ICD-10-CM classification system, it directly impacts medical necessity, reimbursement, and claim approvals.
Understanding ICD-10 Code R51
Historically, ICD-10-CM code R51 represented a general “Headache”. Today, the classification has been refined to include:
- R51.0 – Headache with orthostatic component
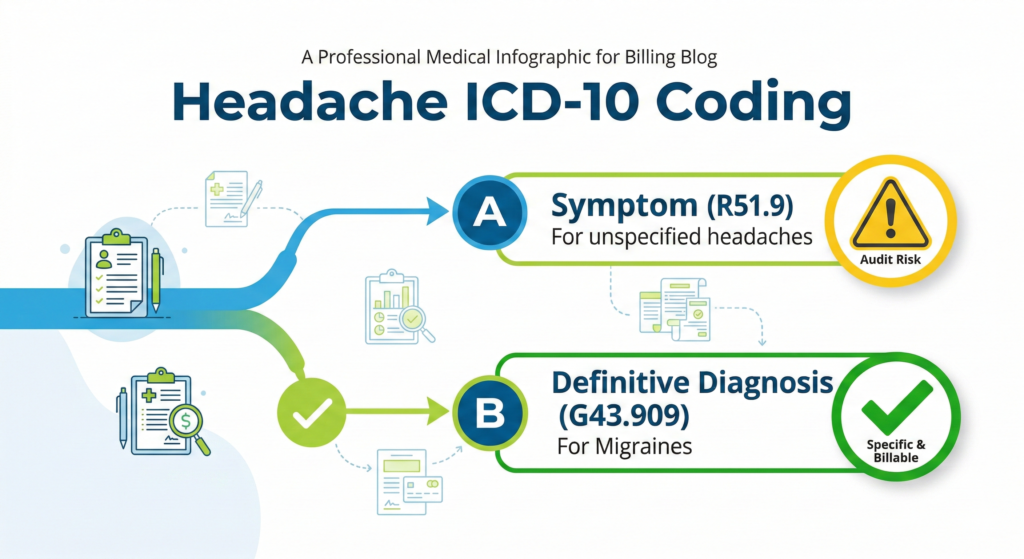
- R51.9 – Headache, unspecified
Headaches are classified under Chapter 18 of ICD-10-CM: Symptoms, Signs, and Abnormal Clinical and Psychological Findings. This means R51 codes describe symptoms, not definitive neurological diagnoses.
When to Use R51 vs. Chapter 6 Codes
Code R51 should only be used when the provider has not determined a specific headache type. If a patient presents with diffuse head pain and no diagnostic conclusion is reached, R51.9 may be appropriate.
However, if the provider documents a definitive diagnosis such as a Migraine, Cluster headache, Tension-type headache, or Post-traumatic headache, symptom coding is no longer correct. You must code the definitive diagnosis from Chapter 6 (Diseases of the Nervous System).
For example, if a provider diagnoses an unspecified migraine without aura, the correct code is G43.909. Using R51 instead is inaccurate and may negatively affect reimbursement.
Clinical Documentation Requirements
Accurate coding begins with robust documentation. Providers must clearly record:
- Onset (sudden vs. gradual)
- Duration
- Location (frontal, occipital, unilateral)
- Severity
- Associated symptoms (nausea, visual changes, photophobia) and aggravating/relieving factors
Common Headache Billing Errors (And How to Fix Them)
1. Overusing R51.9 (Headache, Unspecified)
Repeated use of unspecified symptom codes is a major red flag for insurers. If 70-80% of your headache claims use R51.9, payers influenced by Centers for Medicare & Medicaid Services policies may review your documentation quality. The Fix: Train providers to clearly document the headache type (e.g., Migraine, Tension-type) so coders do not default to assumptions.
2. Ordering Imaging Without Strong Medical Necessity
CT scans and MRIs drive revenue, but they also drive denials. Payers expect clear documentation of “red flags” before approving advanced imaging.
The Fix: Ensure documentation supports medical necessity by noting red flags such as:
- Sudden onset
- Neurological deficits
- Head trauma
- History of cancer or signs of infection
3. Incorrect E/M Level Selection
Under current E/M guidelines, level selection depends on medical decision-making or time. If a provider reviews prior imaging, adjusts medication, discusses risks, and evaluates new symptoms, the visit likely supports moderate complexity. If the note simply says “continue medication,” it supports a lower level. The Fix: Educate providers on documenting the number of problems, data reviewed, and the risk of management decisions.
Stop Billing Errors Before They Impact Revenue
Accurate headache coding demands proper documentation, correct diagnosis selection, and E/M alignment. Medivantek Medical Billing Services helps healthcare providers strengthen revenue performance through accurate ICD-10 & CPT coding alignment and end-to-end Revenue Cycle Management (RCM).
Schedule a Free Billing Assessment with Medivantek Medical Billing Services to discover opportunities to improve reimbursement accuracy and reduce claim denials.