Insomnia is not just a complaint about poor sleep. In clinical practice, it often sits at the center of mental health disorders, chronic pain, neurological issues, and even cardiometabolic risk.
From a billing standpoint, it is equally layered. One wrong code, one vague note, and reimbursement can slip through your fingers.
Sleep disorders are classified under ICD-10-CM, maintained by the Centers for Disease Control and Prevention and enforced in payment systems regulated by the Centers for Medicare & Medicaid Services. That means coding insomnia correctly is not optional. It directly impacts medical necessity, claim approval, and audit exposure.
This guide discusses insomnia billing and coding to enable providers receive proper and timely reimbursements.
Understanding Insomnia ICD-10-CM
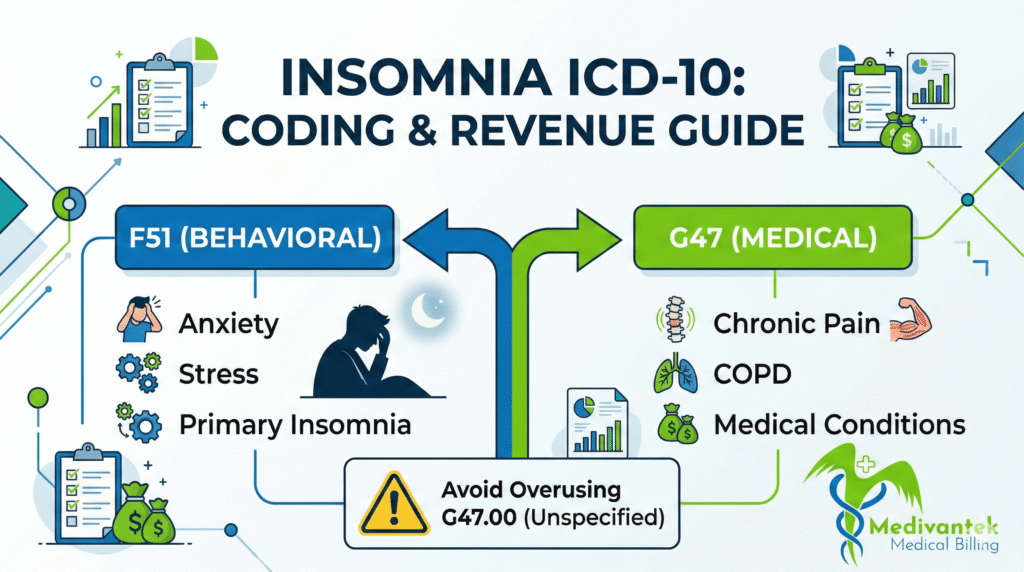
Insomnia appears in two primary sections of ICD-10-CM, and this is where many practices stumble.
First, there is the F51 category. This section falls under “Mental, Behavioral, and Neurodevelopmental Disorders.” These codes apply when insomnia is not due to a substance or known physiological condition and is often behavioral or psychological in origin.
Common codes include:
- F51.01- Primary insomnia
- F51.03- Paradoxical insomnia
- F51.04-Psychophysiologic insomnia
- F51.09-Other insomnia not due to a substance
Then we have the G47 category under “Diseases of the Nervous System.” The most commonly used code here is:
- G47.00- Insomnia, unspecified
- G47.01-Insomnia due to medical condition
- G47.09-Other insomnia
So which one should you use? That answer depends entirely on documentation.
Sleep disorders affect roughly 30% of adults at some point, with chronic insomnia impacting approximately 10-15% of the U.S. population. That translates into millions of outpatient visits annually.
Healthcare spending related to sleep disorders runs into billions of dollars each year, including physician visits, sleep studies, medications, and behavioral therapy.
Given this volume, insurers closely monitor billing trends.
Practices that maintain coding precision and documentation quality outperform competitors in revenue retention.
F51 vs G47 – Choosing the Correct Code
This is where billing accuracy either shines or falls apart.
If the provider documents insomnia linked to anxiety, depression, stress response, or psychophysiologic patterns, F51 codes generally apply.
If insomnia results from a medical condition like chronic pain, COPD, or neurological disorders-G47.01 may be appropriate.
If the documentation is vague and only states “insomnia,” coders often default to G47.00. However, relying on unspecified codes repeatedly raises red flags with payers.
Here’s the golden rule: Code what the provider documents. Not what you assume. If anxiety causes insomnia and both are documented clearly, you may report both diagnoses depending on payer guidelines and clinical relevance.
Clinical Documentation Requirements
Documentation drives coding. Coding drives reimbursement. It’s that simple.
A strong insomnia note should include:
- Duration (acute vs chronic)
- Frequency (nights per week)
- Contributing factors
- Daytime impairment
- Treatment history
- Underlying medical or psychiatric conditions
Chronic insomnia is generally defined as symptoms occurring at least three nights per week for three months or longer. If the provider does not document chronicity, you cannot code it as chronic.
Also, documentation should clarify whether insomnia is:
- Primary
- Secondary to a medical condition
- Substance-induced
- Behavioral
Without this clarity, coders default to unspecified categories.
Unspecified codes often lead to lower reimbursement or medical necessity reviews.
Step-by-Step Billing Process for Insomnia
Let’s break the workflow down the way experienced RCM teams handle it.
1. Insurance Verification
Behavioral health coverage varies widely across plans. Before the visit, verify:
- Mental health benefits
- Deductibles and copays
- Authorization requirements
- Telehealth eligibility (if applicable)
Commercial carriers often carve out behavioral health benefits to third-party administrators. Missing this detail can delay payment.
2. Accurate Coding
Once the visit is completed, review documentation thoroughly. If the provider performs only an evaluation and management (E/M) service, pair the correct ICD-10 code with the appropriate CPT E/M code (99202-99215 for office visits, depending on complexity). If psychotherapy is provided, CPT codes like 90832, 90834, or 90837 may apply. Diagnosis codes must justify these services. Time documentation becomes critical here.
3. Claim Submission
Submit claims electronically with:
- Correct diagnosis pointer linking
- Proper modifiers (if telehealth or prolonged services apply) Accurate provider taxonomy
Missing diagnosis linkage between CPT and ICD-10 is a common cause of denial.
4. Payer Adjudication
Commercial carriers may request:
- Clinical notes
- Proof of chronicity Treatment history
Medicare reviews medical necessity under established LCDs (Local Coverage Determinations). Insomnia alone may not justify high-level services without documented complexity.
5. Denial Management
If denied for medical necessity:
- Review whether underlying conditions were documented but not coded Check if unspecified code was used
- Submit the corrected claim or appeal with detailed notes
A well-written appeal citing documentation often reverses insomnia-related denials.
Medicare Billing Guidelines
Medicare adheres to strict medical-necessity standards under the MPFS (Medicare Physician Fee Schedule).
Reimbursement depends on:
- CPT code level
- Documented medical decision-making
- Diagnosis specificity
For example: A straightforward insomnia medication refill with a stable condition is likely low complexity.
However, chronic insomnia with medication adjustments, comorbid depression, and risk assessment support higher complexity E/M coding.
Sleep studies (CPT 95810 or 95811) require strong medical necessity documentation. Insomnia alone may not always justify polysomnography unless obstructive sleep apnea or other sleep disorders are suspected.
Commercial and Medicaid Considerations
Commercial payers increasingly use predictive analytics. High usage of G47.00 without specificity may trigger audits.
Many plans require prior authorization for:
- Sleep studies
- Behavioral therapy beyond certain sessions
- Certain sedative medications
Medicaid programs vary by state. Some require behavioral health referrals before approving treatment.
Always review payer-specific policies before submitting a claim.
RVUs, Fee Schedules, and Revenue Impact
Under MPFS, E/M codes carry assigned Relative Value Units (RVUs). Complexity documented in the note determines which code level applies.
If documentation underrepresents insomnia severity, practices lose revenue.
For example:
- Low complexity visit (99213 equivalent) carries lower RVUs.
- A moderate complexity visit (99214 equivalent) reimburses significantly more.
Failing to document risk factors, medication adjustments, or functional impairment leaves money on the table.
Errors in Insomnia ICD-10 Billing and How to Avoid Them
Insomnia billing looks simple. A patient cannot sleep. The provider documents insomnia. The claim goes out. Payment should come in. But in reality, that rarely plays out that way. Sleep-related claims sit at the intersection of behavioral health, neurology, and primary care. Because of that, they face closer scrutiny from payers, especially under policies influenced by the Centers for Medicare & Medicaid Services and coding standards maintained by the Centers for Disease Control and Prevention.
Overusing G47.00 (Insomnia, Unspecified)
This is the most common mistake across outpatient practices. Coders default to G47.00 because it feels safe. The documentation only says “insomnia,” so they submit it. The claim gets paid once. Maybe twice. Then the payer analytics system begins to notice a pattern. Repeated unspecified coding signals one of two things to insurers: Either the provider is not documenting thoroughly, or the practice is not coding precisely. Over time, this can trigger medical necessity reviews. Commercial carriers increasingly track trends in unspecified diagnoses. Medicare contractors do the same.
How to avoid it: Train providers to document the type clearly. Is it psychophysiologic? Anxiety-related? Due to chronic pain? Acute? Chronic? Even a single clarifying sentence in the assessment section can allow the coder to assign a more specific ICD-10 code. Specificity reduces audit risk and strengthens medical necessity.
Failing to Code the Underlying Condition
Insomnia is often secondary. Anxiety disorders, depression, chronic pain, PTSD, and neurological diseases frequently cause sleep disturbances. If the provider addresses both insomnia and the underlying condition, but the coder submits only insomnia, the claim underrepresents the visit complexity. This affects reimbursement. It can also weaken medical necessity for higher-level E/M codes or therapy services. For example, A patient with major depressive disorder presents with worsening insomnia. Medication is adjusted. Risk assessment is documented. If only insomnia is coded, the payer may downcode the visit.
How to avoid it: Always code documented comorbidities that are evaluated, assessed, or managed during the encounter. Follow ICD-10 guidelines carefully. Diagnosis coding should reflect the full clinical picture, not just the symptom.
Coding Chronic Insomnia Without Documentation
Another frequent issue is assuming chronicity. Chronic insomnia typically means symptoms occur at least three nights per week for three months or more. If the provider does not state chronic, you cannot code chronic. Coders sometimes infer based on history. That is risky. Auditors review what is written, not what is implied.
How to avoid it: Encourage providers to state the duration clearly. If it is chronic, document the timeline. If it is acute, say so. That one detail changes coding accuracy.
Inadequate Medical Decision-Making Documentation
Insomnia visits often involve medication management. Sedative-hypnotics, antidepressants, melatonin agonists, or behavioral therapy referrals are common.
Yet many notes fail to reflect the risk involved in prescribing or adjusting these medications.
Without clear documentation of:
- Risk discussion
- Side effect monitoring Alternative treatments
- Follow-up plan
The visit may not justify a moderate or high-level E/M code.
Under the Medicare Physician Fee Schedule (MPFS), medical decision-making drives reimbursement. Poor documentation equals lost RVUs.
How to avoid it:
Document risk. Document medication adjustments. Document monitoring plans. Spell out the complexity. It protects revenue and compliance.
Missing Time Documentation for Psychotherapy
If psychotherapy is billed alongside insomnia treatment, time documentation becomes critical. CPT codes for therapy require clear time statements. Without them, claims are vulnerable. Payers frequently request records for behavioral health services. If time is not documented, repayment may be demanded.
How to avoid it: Ensure the provider documents total time spent in therapy and that it meets CPT thresholds. Review notes before submission.
Ignoring Payer-Specific Authorization Rules
Commercial payers often require prior authorization for sleep studies or extended behavioral therapy sessions. Submitting claims without authorization leads to immediate denial. Appeals rarely succeed in these cases. Medicaid policies vary by state. Some require referrals before approving certain sleep-related services.
How to avoid it: Verify benefits before services are rendered. Confirm authorization requirements. Build this into your front-desk workflow.
Linking the Wrong Diagnosis to the CPT Code
Diagnosis pointer errors are more common than people think. If a psychotherapy CPT code is linked only to G47.00 instead of the documented anxiety disorder driving treatment, the claim may fail medical necessity review.
How to avoid it: Review claim forms carefully. Ensure the diagnosis pointer matches the service rendered. Double-check before electronic submission.
Poor Follow-Up Documentation
Chronic insomnia management requires continuity.
If follow-up visits show no documented progress, no medication review, and no updated assessment, payers may question the medical necessity for repeated visits. Patterns matter. Payers analyze utilization trends.
How to avoid it: Encourage providers to document response to treatment, symptom changes, and care plan adjustments at each visit.
Final Thoughts
Insomnia coding demands attention to detail. It touches behavioral health, neurology, and primary care. It affects medical necessity, RVUs, and compliance audits.
When documentation is strong, coding becomes straightforward. When documentation is vague, denials follow.
Specificity protects reimbursement. Accuracy protects compliance. And consistency protects long-term revenue.
That is how experienced billing professionals handle ICD-10 coding for insomnia the right way.
Struggling with Insomnia Claim Denials or Documentation Issues?
Accurate insomnia coding requires more than selecting an ICD-10 code. It demands precise documentation, correct diagnosis linkage, payer compliance, and proactive denial management.
Medivantek Medical Billing Services helps healthcare providers optimize sleep disorder billing through:
- Accurate ICD-10 & CPT coding
- Behavioral health billing expertise
- Medical necessity compliance
- Denial prevention and appeals management
- Revenue cycle optimization
Schedule a Free Billing Consultation today and discover how much revenue your practice may be losing due to coding inefficiencies.
📞 Contact Medivantek Medical Billing Services to improve reimbursements and reduce claim denials.