Insomnia is not just a complaint about poor sleep. In clinical practice, it often sits at the center of mental health disorders, chronic pain, neurological issues, and cardiometabolic risk. From a billing standpoint, it is equally layered. One wrong code or vague note can cause reimbursement to slip through your fingers.
Sleep disorders are classified under ICD-10-CM, enforced in payment systems regulated by the Centers for Medicare & Medicaid Services. Coding insomnia correctly directly impacts medical necessity, claim approval, and audit exposure.
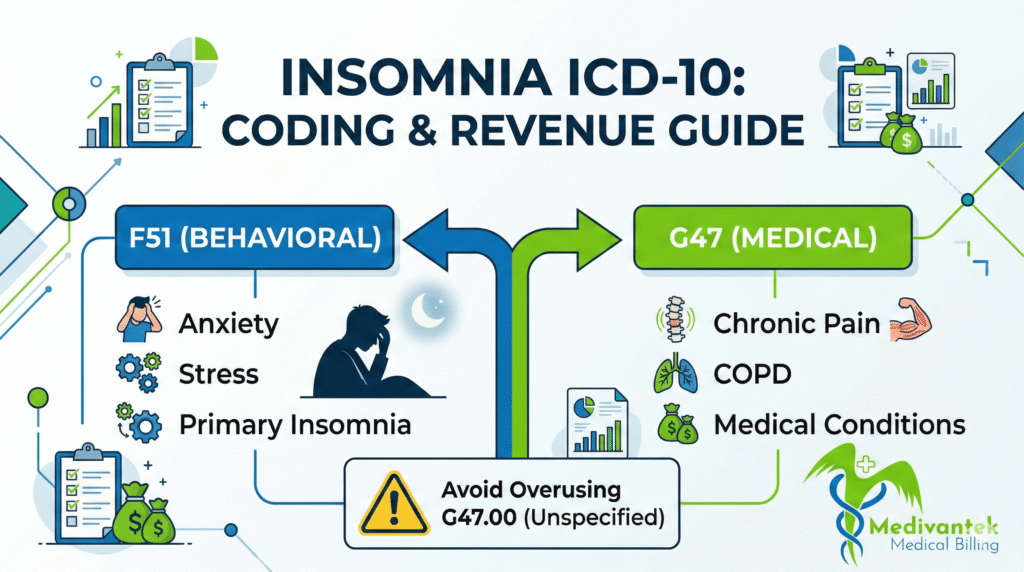
Choosing the Correct Category: F51 vs. G47
Insomnia appears in two primary sections of the ICD-10-CM, which is where many practices stumble.
1. The F51 Category (Mental & Behavioral Disorders)
These codes apply when insomnia is not due to a known physiological condition or substance, and is often psychological in origin. Common codes include:
- F51.01 – Primary insomnia
- F51.04 – Psychophysiologic insomnia
2. The G47 Category (Diseases of the Nervous System)
These are used when insomnia results from a physiological medical condition like chronic pain or COPD. Common codes include:
- G47.01 – Insomnia due to medical condition
- G47.00 – Insomnia, unspecified
The Golden Rule: Code what the provider documents, not what you assume.
Clinical Documentation Requirements
Documentation drives coding, and coding drives reimbursement. To support medical necessity, a strong insomnia note must include:
- Duration (acute vs. chronic)
- Frequency (nights per week)
- Daytime impairment and contributing factors
- Treatment history and underlying medical or psychiatric conditions
For example, chronic insomnia is generally defined as symptoms occurring at least three nights per week for three months or longer. If the provider does not document chronicity, you cannot code it as a chronic condition.
Common Insomnia Billing Errors (And How to Fix Them)
1. Overusing G47.00 (Insomnia, Unspecified)
This is the most common mistake across outpatient practices. Coders default to G47.00 because the documentation only says “insomnia”. While the claim might get paid initially, repeated unspecified coding triggers medical necessity reviews and signals to payers that your documentation is lacking. The Fix: Train providers to clearly document the type and cause of the insomnia to allow for specific ICD-10 assignment.
2. Failing to Code the Underlying Condition
Insomnia is often secondary to anxiety, depression, PTSD, or chronic pain. If the provider evaluates both the insomnia and the underlying condition, but the coder only submits the insomnia code, the claim underrepresents the visit’s complexity. The Fix: Always code documented comorbidities that are evaluated or managed during the encounter.
3. Inadequate Medical Decision-Making (MDM) Documentation
Insomnia visits often involve prescribing or adjusting sedative-hypnotics, antidepressants, or melatonin agonists. Without clear documentation of the risk discussion, side effect monitoring, and alternative treatments, the visit may not justify a moderate or high-level E/M code (like a 99214). The Fix: Clearly document medication risks, adjustments, and monitoring plans to protect your RVUs and compliance.
Stop Insomnia Billing Errors Before They Impact Revenue
Accurate insomnia coding requires precise documentation, correct diagnosis linkage, payer compliance, and proactive denial management.
Medivantek Medical Billing Services helps healthcare providers optimize sleep disorder billing through accurate ICD-10 & CPT coding, behavioral health billing expertise, and end-to-end revenue cycle optimization.
Schedule a Free Billing Consultation today and discover how much revenue your practice may be losing due to coding inefficiencies.